
10
Feb
Accelerated Breast Cancer Radiation Therapy
Dr Vineeta Goel, Director, Radiation Oncology, Fortis Hospital, Shalimar Bagh
Breast cancer treatment has undergone considerable evolu...

10
Feb
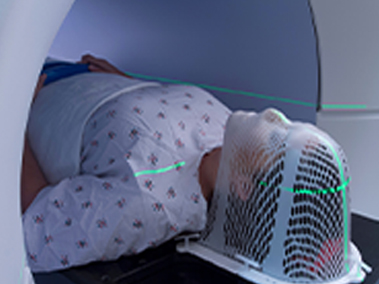
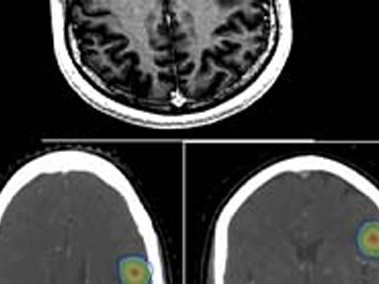
Stereotactic Radiation Therapy For Brain Metastases
Case 1 -Single Brain Metastases
A 55 Years old lady was diagnosed with left breast cancer in August 2015. She was treated with breast ...

10
Feb
Radiation Therapy For (Left) Breast Cancer With Cardiac / Heart Protection
Breast Cancer is one of the most common cancers among women. Good news is, that many more patients today are long term breast cancer “s...

10
Feb
Breast Cancer Radiation Therapy
Radiation Therapy (RT) for breast cancer has seen a long journey precision and focused therapy. RT is an important part of breast cance...
10
Feb
Stereotactic Radiotherapy
Conventional radiation therapy for cancers often results in some collateral damage to nearby healthy tissues. Stereotactic Radiotherapy...

10
Feb
Stage IV Breast Cancer With Paralysis Of Lower Limbs
A 48 years old woman presented to us with paralysis of 4 days duration. She also gave a history of upper backache since past 5 months. ...

10
Feb
Total Skin Electron Beam Therapy
Total Skin Electron Beam Therapy (TSET) is a radiation technique which is used to treat patient’s entire/total skin surface using elect...
10
Feb
Solitary Brain Metastases From Breast Cancer-Treatment With Stereotactic Radiation Therapy
A 54 Years old lady was diagnosed with left breast cancer in August 2015. Her breast biopsy confirmed it to be Invasive Ductal Carcinom...

10
Feb
Intra Operative Radiation Therapy (IORT) With Brachytherapy
Intraoperative radiation therapy (IORT) is single dose of focused radiation therapy delivered at the time of surgery.
Brachytherapy is...

10
Feb
Management Of Intracranial Non Germinomatous Germ Cell Tumour (Choriocarcinoma) Brain With Chemotherapy And Cranio Spinal Radiation Therapy
18 Years old college student presented to hospital with complaints of severe headache, blurring of vision, vomiting and episode of unco...

10
Feb
Stereotactic Radiotherapy For Brain Metastases
Spread of cancer to brain called as brain metastases is known to occur in few cancers. All patient with brain metastases require radiat...

10
Feb
Heart Sparing Radiation Therapy
Heart Sparing Radiation Therapy for (Left) Breast Cancer
Breast cancer is one of the most common cancers among women. Good news is, ...

10
Feb
Carcinoma Cervix With Intrauterine Fibroids
56 years old lady with no comorbidities was investigated for postmenopausal bleeding PV. Clinically she had growth involving cervix wit...
10
Feb
Stage IV Breast Cancer With Paralysis Of Lower Limbs
A 48 years old woman presented to us with paralysis of 4 days duration. She also gave a history of upper backache since past 5 months. ...

10
Feb
Radiation Therapy In Cancer Management
What is Radiation Therapy and what does it do?
Radiation Therapy is use of high energy Ionization radiation (often X Rays ) to kill a ...

10
Feb
Post mastectomy pain—Less discussed but common problem
Mastectomy can be associated with some annoying symptoms like
Tightness around the chest
Chronic chest pain
Stiffness and re...
10
Feb
Left Breast Cancer Radiation Therapy Respiratory Gating To Save Heart
Safety of modern breast RT for lungs and heart
Modern Radiation therapy with IMRT/IGRT is much safer
Small risk of cardiac ds (5-6%...

10
Feb
Breast Cancer Radiation Therapy- Journey From 5 Weeks to 5 Days Treatment
Radiation Therapy (RT) for breast cancer has seen a long journey precision and focused therapy. RT is an important part of breast cance...

10
Feb
Intraoperative Radiotherapy
Intraoperative radiation therapy (IORT) is a form of precise and impactful radiation therapy. IORT refers to a single shot of high dose...
10
Feb
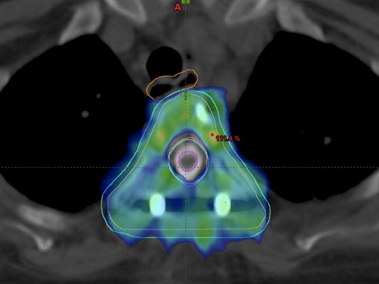
Interstitial / Intracavitary Brachytherapy For Cervical Cancer
Brachytherapy is a boon of medical science for patients having cervical cancer.
And it needs deep knowledge and extensive equipment fo...