View Large
View Large

56 years old lady with no comorbidities was investigated for postmenopausal bleeding PV. Clinically she had growth involving cervix with bulky uterus and bilateral parametrium medially infiltrated by disease. Biopsy from cervical mass showed moderately differentiated squamous cell carcinoma. Contrast MRI abdomen showed bulky cervical mass with multiple subserosal, submucosal and intramural fibroids with largest fibroid measuring 8.6 x 7cm. There was no lymphadenopathy; both liver and kidneys were normal. Her Chest X-ray was unremarkable.
Diagnosis
Her final diagnosis was squamous cell carcinoma cervix FIGO stage II B with multiple large intra uterine fibroids.
Management
Standard of care for this stage cervical carcinoma is concurrent chemotherapy and external beam radiation therapy for 5 weeks followed by intracavitary brachytherapy. The challenge before us in this was the large intra uterine fibroids would prevent successful placement of intracavitary brachytherapy applicator. Surgery was already ruled out due to bilateral medial parametrium infiltration by disease.
After discussion in multispeciality tumour board we decided to treat this patient with 5 weeks of concurrent chemoradiotherapy (CTRT). She received weekly Injection Cisplatin 35 mg/m2 along with 45 Gy/25 Fractions of radiation therapy to cervix, uterus and pelvic lymph nodes with image guided Intensity Modulated Radiation Therapy (IG- IMRT).
Patient tolerated CTRT well and clinically had >80% regression in cervical mass. Repeat MRI at completion of CTRT also showed >80 disease regression with small residual diseases with bilateral medial parametrium infiltration.
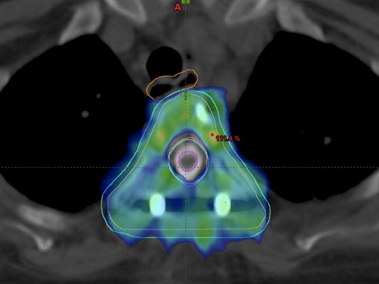
The patient was next taken up for Interstitial Brachytherapy along with intra uterine tube placement under USG guidance. USG helped us navigate our needles and tubes in correct position despite multiple large obstructing intrauterine fibroids. This whole procedure was done under spinal anesthesia with epidural catheter for maintain analgesia. Patient with stood this procedure well.
Follow Up
Post treatment she has a follow up of one year and she is disease free.
Discussion
Radiation Therapy has been the treatment modality of choice for management of cancer cervix for more than a century. In last two decades radiation therapy with weekly concurrent chemotherapy (CTRT) has become the new standard of care.
Success of radiation therapy in providing high cure rates in carcinoma cervix is essentially due to use of brachytherapy. Brachytherapy allows us to give high doses of radiation inside tumour region with very less radiation dose to surrounding normal organs. Treatment of carcinoma cervix remains incomplete without brachytherapy. Presence of intrauterine fibroids is considered a relative contraindication for treating patients with radiation therapy as brachytherapy is generally not feasible. In this patient, we could manage successful brachytherapy as we used intraoperative USG guidance and we replaced traditional intracavitary brachytherapy with interstitial procedure. Interstitial brachytherapy gives us more freedom using needles to adequately cover the entire tumour with adequate radiation doses.