View Large
View Large

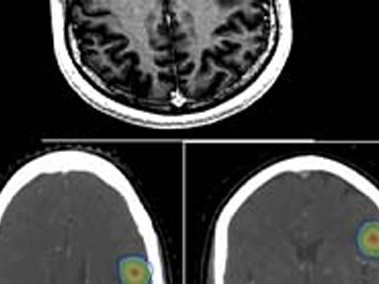
18 Years old college student presented to hospital with complaints of severe headache, blurring of vision, vomiting and episode of unconsciousness. Clinically patient was conscious, alert but very irritable with normal sensory motor function. He underwent initially CT Head followed by contrast MRI Brain which showed 30x 41 x 39 mm heterogeneous lesion in posterior aspect of third ventricle with contiguous parenchymal infiltration with radiological diagnosis of pineal germ cell tumour.
Subsequently his serum ß HCG was found to be 1, 11, 505 mIU and AFP of 1.36 ng/ml. He underwent CSF sampling which showed no malignant cells on cytology with CSF ß HCG of 1, 40, 614 mIU/ml and AFP of <0.5 ng/ml. His MRI Spine screening was also normal.
Diagnosis
Based on his radiological picture coupled with raised serum and CSF ß HCG with normal AFP, diagnosis of Primary CNS non seminomatous germ cell tumour (NSGCT) with subtype Choriocarcinoma was made.
Management
Patient initially underwent VP shunt control symptoms of raised intracranial pressure and was then started on chemotherapy. After completing four cycles of chemotherapy his serum and CSF ß HCG decreased significantly to 8.4 and 68.6 mIU/ml respectively. His repeat MRI Brain showed much smaller residual disease. Patient also showed much improvement symptomatically.
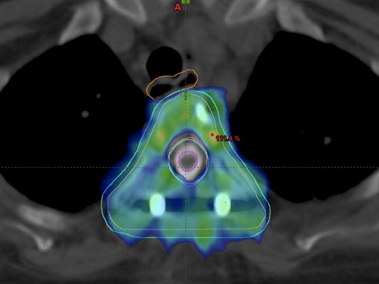
He was then treated with Cranio Spinal Irradiation (CSI) with Intensity Modulated Image Guided Radiation Therapy (IM IGRT) to a dose of 30.6Gy in 17 fractions followed by local tumour boost to 19.8Gy over 11 fractions. This whole treatment was carried out on TruBeam STX Linear Accelerator at Max Hospital, Shalimar Bagh. Patient tolerated CSI radiation therapy well with grade II haematological and grade I GI toxicity. Patient completed his entire treatment in July 2018.
Follow up
Patient has been on regular follow up for last 18 months and his diseases remains in remission clinically, radiologically and biochemically and he has resumed back his studies in college.
Discussion
Primary Choriocarcinoma of brain is a rare tumour. Biopsy is generally not mandatory for its confirmation as diagnosis is generally made by combination of radiological picture along with raised serum and CSF ß HCG. Surgical resection of tumour is also generally not required as this tumour is very chemo and radio sensitive. Response to treatment is generally done by repeating serum and SCF ßHCG values which should show declining values.
Radiation therapy target for NSGCT Brain includes entire brain and spinal axis including leptomenninges and is termed as cranio spinal radiation. It’s a large and irregular target volume spanning almost across patient’s whole body. Covering cranio spinal axis with radiation therapy also comes with challenge of sparing all organs of body (lung, heart, kidney, esophagus) and cranial structures like eyes, lens, cochlea etc.
With present radiation therapy techniques, it is possible to treat this irregular target volume of brain and spine using combined technique of intensity modulated image guided radiation therapy (IM- IGRT). IMRT helps us to focus radiation doses at correct region while saving adjacent normal organs. IGRT involves using on board Cone beam CT Scan to verify patient positioning every day before radiation therapy.