View Large
View Large

A 54 Years old lady was diagnosed with left breast cancer in August 2015. Her breast biopsy confirmed it to be Invasive Ductal Carcinoma (IDC) with strong positivity for hormonal receptors (Estrogen and Progesterone) and negativity for Her 2 Neu (Epidermal Growth Factor Receptor). She underwent Left Breast Conservation surgery followed by chemotherapy and Radiation Therapy. After completion of radiation therapy, she was started on oral hormonal therapy treatment – in form of daily tablets.
She remained disease free for 34 months (2 years 10 months), when in October 2018, she had an episode of seizure. Clinically she was well preserved with ECOG performance status of 1, breast cancer was clinically controlled and she was neurologically intact. Contrast MRI Brain showed 1.5×1.4 x1.6 cm intensely enhancing nodule in left posterior frontal region with mild surrounding edema suggestive of solitary brain metastases. MR Spectroscopy showed intense choline peak with reduced NAA suggestive of mitotic etiology. Patient also underwent FDG whole body PET CT scan which showed that brain was the only site of metastases.
Diagnosis
Her final diagnosis was Solitary Brain Metastases from Left Breast Cancer after disease free interval of 34 months in a 54 years old well preserved lady.
Management
Patient was evaluated for surgical resection with the idea that it would also give histo biopsy specimen to repeat hormonal and other IHC markers profile to decide systemic treatment. Her functional MRI brain showed motor activation area in close proximity to metastases and Broca’s area close to FLAIR abnormality. Neurosurgical resection of brain lesion was ruled out in view of location in close vicinity of motor and speech area.
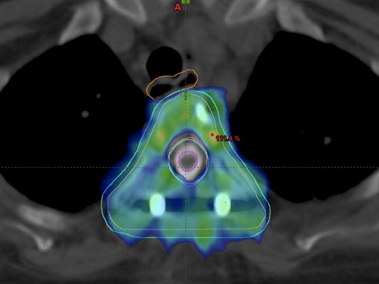
She was then treated with stereotactic brain radiation therapy. He head was fixed in a non- invasive frame/mould. Since her lesion was lying in eloquent area (close to motor and speech cortex), her radiation therapy (RT) was delivered in 3 fractions instead of single fraction RT. She was treated with 27Gy in 3 fractions to brain metastases using stereotactic radiosurgery (SRS) technique under image guidance.
After brain radiosurgery her hormonal treatment was changed in form of another pill. She was not given chemotherapy as her previous breast cancer was hormone receptor positive.
Follow up
Post brain SRS, patient has a follow up of one year 3 months (15 months) and she is disease free. She has no neurological deficit and she continues to be on hormonal treatment. Her repeat MRI Brain showed small residual non enhancing lesion of 6×7 mm and there are no new cranial or extracranial lesions.
Discussion
In past decade, there has been a major shift in approach to management of metastatic cancers with an attempt to potentially cure especially oligo (few/limited) and solitary metastases. This potentially curative treatment approach requires systemic treatment along with aggressive local treatment of metastases either with surgery or ablative high dose radiation therapy with stereotactic approaches (SRS or SBRT).
Till few years back standard treatment of brain metastases was whole brain radiation therapy (WBRT). A new standard of care for brain metastases is to give focal stereotactic radiation therapy. There are several advantages of SRS over WBRT including short treatment, better local control of metastases, no neurocognition decline and no hair loss.