View Large
View Large

Conventional radiation therapy for cancers often results in some collateral damage to nearby healthy tissues. Stereotactic Radiotherapy (SRT) is defined as a method of external beam radiotherapy that use principles of stereotaxy to accurately deliver high radiation dose to a tumour/ target in one or few treatment fractions (1 to 5) without much radiation dose and side effects to the surrounding healthy tissues.
When this technique is used to treat brain tumours (primary /secondary) then it’s called as Stereotactic radiosurgery/ radiotherapy (SRS/SRT). While when this same technique is used for treating tumours outside brain/extra cranial , it’s called as SBRT (Stereotactic Body Radiation Therapy).
SRT is used to treat both primary cancers (where the cancer started such as the lung or the prostate), or where a cancer may have spread to other body organs (secondary cancers or metastases). It is also addressed as SABR (Stereotactic ablative radiation therapy), as it involves the delivery of much higher and near ablative doses of radiation to cancer.
How is SRT different from other forms of RT?
• SBRT involves high precision, image guided focused dose deliveredto the target with rapid dose fall off– translates in to higher control rates
• SBRT has highly conformal radiation with rapid dose fall off to avoid/minimize radiation to healthy normal tissues – minimal side effects
• Larger doses per fraction (typically ≥ 8 Gy per fraction) to ablate the tumor- helps in overcoming radioresistance if any
• Fewer treatment fractions (typically 1-5 fractions) as compared to typical of 15-35 fractions in conventional RT
• Intra-fraction motion management wherever applicable for hitting at the accurate target every day with RT
What are the indications of using Stereotactic Radiation Therapy?
SRT can be used at various sites including
- Primary Brain Tumours like Meningioma, Schwannomas etc.
- Secondary Brain Tumour – Brain Metastases
- Medically inoperable early-stage primary lung cancers (T1/2N0MO)
- Lung metastasis (up to 5-8 in number)
- Spine metastasis
- Primary (Hepatocellular Carcinoma) and secondary liver tumours
- Inoperable/recurrent carcinoma pancreas
- Early low risk prostate cancer

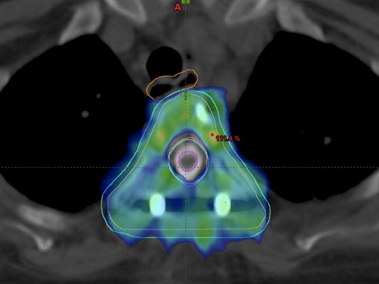
Case1 Carcinoma Cervix Patient with isolated liver metasatses treated with SBRT to liver metastases while sparing rest uninvolved liver
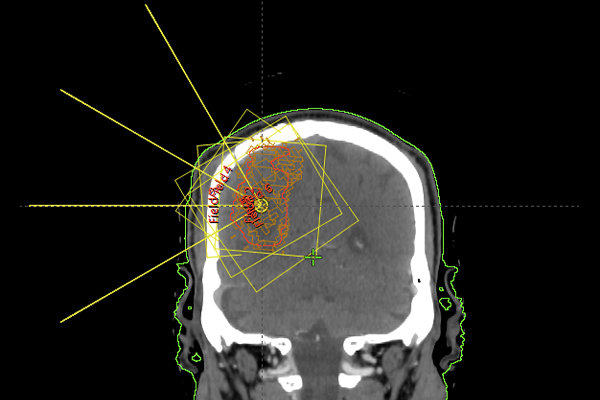
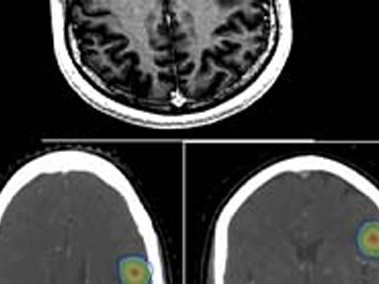
Case 2 –Follow up case of Renal Cell Carcinoma with solitary brain metastases treated with post op SRT to Brain (without whole brain RT)
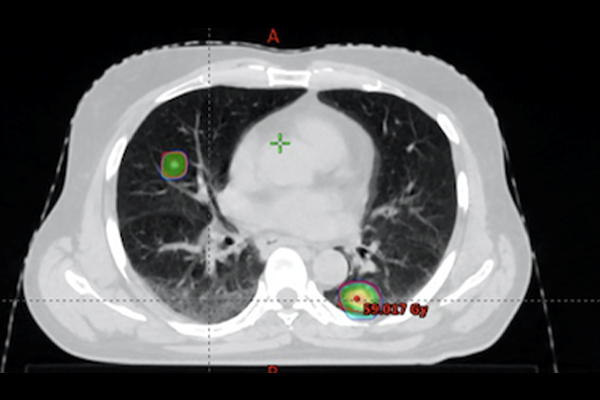
Case 3 – Carcinoma Urinary Bladder patient with Oligo metastases to Lung treated with SBRT with sparing of normal unaffected lungs
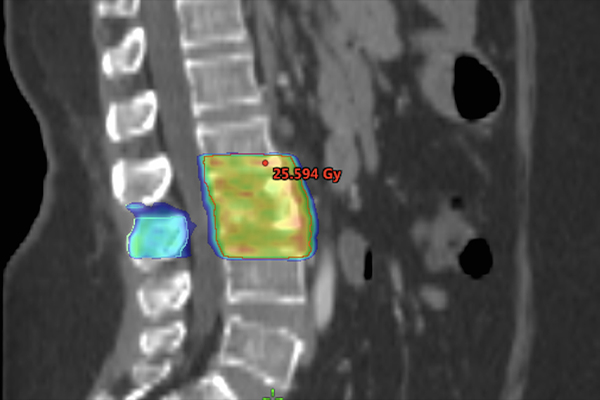
Case 4 Carcinoma Prostate with Spine metastases treated with SBRT to spine
Stereotactic RT delivers high ablative doses precisely to tumour which results in better tumour control and quick symptomatic relief to patients.
Dr. Vineeta Goel, Director Radiation Oncology at Fortis Hospital Shalimar Bagh is the best doctor for STEREOTACTIC RADIOTHERAPY.
# Stereotactic radiation therapy #SRS #SRT #SBRT # Brain Metastases # Liver tumour # Liver Metastases # Spine metastases # Bone Metastases # Lung metastses